Peripheral Blood film in MRCP(2)
I told you a few basic terms used in haematology in my previous post. Today, I will talk about a few common and popular blood films that are commonly asked in MRCP Part 1 and 2.
1) Sickle Cell disease
I told you a few basic terms used in haematology in my previous post. Today, I will talk about a few common and popular blood films that are commonly asked in MRCP Part 1 and 2.
1) Sickle Cell disease
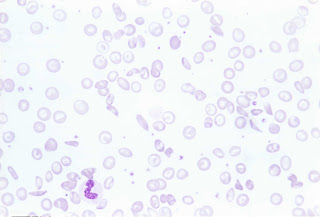 ( Blood film of sickle cell, polychromasia and target cell)
( Blood film of sickle cell, polychromasia and target cell)
By far, I think this the most popular blood film in MRCP. Remember that patients with sickle cell may present with bone pain ( due to bone necrosis), osteomyelitis, leg ulcers or even iron overload. Remember that it is one of the important causes of chronic haemolysis anaemia, therefore, you might find pallor with jaundice in patients with Sickle Cell Disease. However, remember that you may not find splenomegaly ( although you anticipate splenomegaly in patients with chronic haemolysis) because there is a possibility of splenic infarct!!
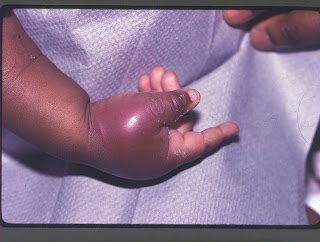 ( Patient presents with painful bony infarction)
( Patient presents with painful bony infarction)2) Thalassemia
This disease needs no further explanation. I have seen so many Thalassemic patients during my paediatric posting when I was a medical student.
Look at the following blood film,
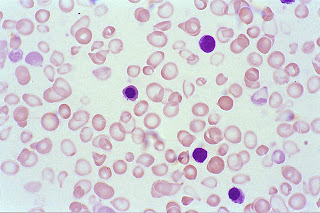 ( Blood film showing hypochromic, microcyctic red cells)
( Blood film showing hypochromic, microcyctic red cells)You may be given a photo of patient with classical thalassemic facies and you are expected to know about types of Thalassemia, chromosome involved and complications!
3) Malaria
OK, if you are living in UK or Ireland, you may not seen a case of malaria in your whole life. However, malaria is endemic in tropical countries including Malaysia and Thailand. You may still remember that there are various species of Plasmodium such as P.falciparum, P.vivax and P.ovale. Anyway, remember that in your MRCP, they always show you the ring form!


