Today I am going to talk about the last part of this important topic- Cardiac Catheterization in MRCP. In my previous two posts, we have learned about some common cases concerning cardiac catherization in MRCP. I am going to show two more cases here,
 Case 1:
Case 1:
Coarctation of the aorta
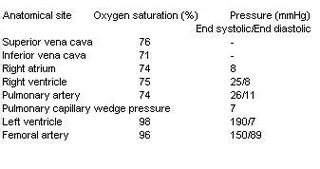
This is an easy case!There is a steep systolic gradient between the left ventricle and the femoral artery; the gradient is calculated as 190 – 150 = 40 mmHg. Therefore the diagnosis is Coarctation of the aorta.
Case 2:
Tetralogy of Fallot
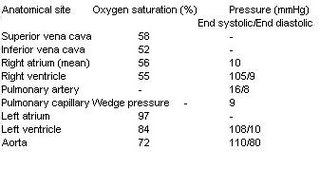
You notice a combination of pressure and oxygen saturation abnormalities. The abnormalities are,
i) Step-down in oxygen saturation between LA and LV, indicating right to left shunt at the level of the ventricles, therefore there is presence of VSD.
ii) Pulmonary stenosis: there is an 89 mmHg gradient across the pulmonary valve (RV systolic – PA systolic).
iii) RVH: Right ventricular pressures are high and there is a right to left shunt, as indicated by the oxygen saturations
Hope you find this information useful. Remember, in MRCP examination, you may be given the result of a cardiac catheterization and asked about the correct physical signs of a patient. In other type of question setting, you maybe given some important physical signs and the examiners want you to find the correct cardiac catheterization results.
 1) it has central and peripheral anticholinergic effects
1) it has central and peripheral anticholinergic effects




 There is a systolic gradient of 81 mmHg across the aortic valve (LV systolic pressure – aortic systolic pressure), indicating severe aortic stenosis. Remember that hypertrophic cardiomyopathy also presents with a similar result, howeve, patients tend to be younger!
There is a systolic gradient of 81 mmHg across the aortic valve (LV systolic pressure – aortic systolic pressure), indicating severe aortic stenosis. Remember that hypertrophic cardiomyopathy also presents with a similar result, howeve, patients tend to be younger!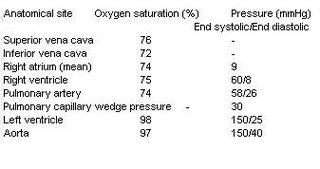 This is an easy case, you notice a wide pulse pressure ( aorta :150/40), therefore the diagnosis is aortic regurgitation.
This is an easy case, you notice a wide pulse pressure ( aorta :150/40), therefore the diagnosis is aortic regurgitation. 


