In sinus rhythm, we know that every P wave is followed by QRS, you must learn hard the following conditions that do not give you sinus rhythm,
1) Atrial fibrillation
This is the commonest condition being asked in MRCP, I have covered this in my previous post.
2) Atrial flutter
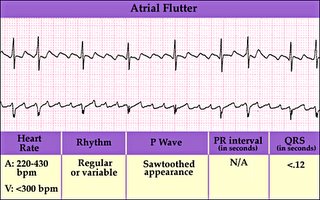
Always described as “ Saw-Tooth” ECG in medical textbook. The atrial activity is usually between 250-350 beats /min and there is sually 2:1 or 3:1 block. Causes for atrial flutter are similar to atrial fibrillation as well as the management.
3) Ventricular tachycardia

Defined as three or more successive ventricular extrasystoles at a rate more than 120/min. Remember than VT has a wide QRS complex. Causes of VT include
a) Ischaemia to the heart
b) Hypo-or hyperkl\alaemia
c) Long QT interval ( a very popular question in MRCP, I will cover this in depth in my future post)
d) Cardiomyopathies
4) Torsades des pointes

Actually it is a type of ventricular tachycardia with a varying axis. It often happens after heart attack but can be due to drugs and other causes of prolonged QT interval.
5) Ventricular fibrillation
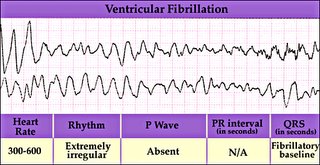
This rhythm needs immediate cardioversion. Usually happens after a hear attack
Important Tips for MRCP,
It is often difficult to differentiate an SVT with abberant ventricular conduction from VT ( both also have wide QRS complexes), however always remember in clinical practice, always assume VT if you are in doubt and treat accordingly because VT is commoner and life threatening. However, following features suggest SVT with abberant blocks,
1) No fusion or capture beats
2) Presence of P waves associated with ORS
3) Classical RBBB and LBBB ORS morphology
4) ORS <0.14s
5) Same QRS morphology as in sinus rhythm
6) Normal axis

No comments:
Post a Comment