Peripheral Blood film in MRCP(2)
I told you a few basic terms used in haematology in my previous post. Today, I will talk about a few common and popular blood films that are commonly asked in MRCP Part 1 and 2.
1) Sickle Cell disease
I told you a few basic terms used in haematology in my previous post. Today, I will talk about a few common and popular blood films that are commonly asked in MRCP Part 1 and 2.
1) Sickle Cell disease
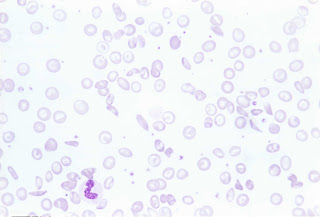 ( Blood film of sickle cell, polychromasia and target cell)
( Blood film of sickle cell, polychromasia and target cell)
By far, I think this the most popular blood film in MRCP. Remember that patients with sickle cell may present with bone pain ( due to bone necrosis), osteomyelitis, leg ulcers or even iron overload. Remember that it is one of the important causes of chronic haemolysis anaemia, therefore, you might find pallor with jaundice in patients with Sickle Cell Disease. However, remember that you may not find splenomegaly ( although you anticipate splenomegaly in patients with chronic haemolysis) because there is a possibility of splenic infarct!!
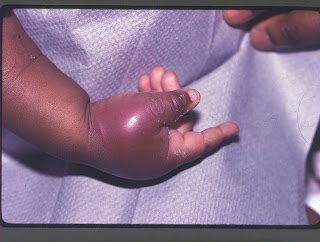 ( Patient presents with painful bony infarction)
( Patient presents with painful bony infarction)2) Thalassemia
This disease needs no further explanation. I have seen so many Thalassemic patients during my paediatric posting when I was a medical student.
Look at the following blood film,
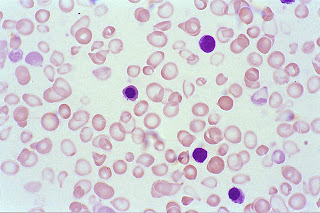 ( Blood film showing hypochromic, microcyctic red cells)
( Blood film showing hypochromic, microcyctic red cells)You may be given a photo of patient with classical thalassemic facies and you are expected to know about types of Thalassemia, chromosome involved and complications!
3) Malaria
OK, if you are living in UK or Ireland, you may not seen a case of malaria in your whole life. However, malaria is endemic in tropical countries including Malaysia and Thailand. You may still remember that there are various species of Plasmodium such as P.falciparum, P.vivax and P.ovale. Anyway, remember that in your MRCP, they always show you the ring form!


1 comment:
United Nations Economic Commission For Africa
Book Of Abstracts
Science With Africa Conference
March 3-7, 2008
page 30
Evaluation of Niprisan (Herbal Medicine) for the Management of Sickle Cell
Anaemia
Charles Wambebe and Hadiza Khamofu, International Biomedical Research in Africa, Abuja,
Nigeria, wambebe@yahoo.com, Joseph Okogun, Nathan Nasipuri and Karynius Gamaniel,
National Institute for Pharmaceutical Research and Development, Abuja, Nigeria.
About 70% of all sickle cell anemia (SCA) subjects reside in Africa, estimated at over 12 million. The prevalence of SCA is estimated at over 2% while infant mortality is about 8% and survival rate of SCA babies in rural areas by five years of age is about 20%. These statistics indicate that SCA is probably the most neglected (and sometimes forgotten by health authorities) serious public health disorder with serious mortality and morbidity rates in Africa. The objective was to undertake pre-clinical and clinical assessments of a herbal extract vis-à-vis management of sickle cell anemia using Good Laboratory Practice and Good Clinical Practice principles respectively. In Africa, there is no standard treatment for sickle cell anemia, only palliative management is generally available. In view of this situation, most SCA subjects use herbal medicines. NIPRISAN is a standardized extract from four medicinal/food plants: Piper guineenses seeds, Pterocarpus osun stem, Eugenia caryophyllum fruit and Sorghum bicolor leaves. Short term toxicity study indicated that NIPRISAN was safe in laboratory animals. Bio-activity guided fractionation show that vanillin and aromatic aldehydes may be the bioactive moieties. NIPRISAN reversed sickled red blood cells and
protected them from being sickled when exposed to low oxygen tension. NIPRISAN dose-dependently delayed polymer formation of haemoglobin S. NIPRISAN induced 85% increased solubility of deoxy haemoglobin S. The in vivo efficacy study was undertaken at Children Hospital of Philadelphia, USA. Histological examination of lungs of control Tg transgenic mice carrying human sickle haemoglobin showed entrapment of massive numbers of sickled cells in alveolar capillaries. NIPRISAN significantly cleared the lungs of sickled cells. Furthermore, NIPRISAN induced profound effect on the survival time of Tg mice under hypoxic conditions (p<0.0001). The phase II clinical data indicated that all the subjects benefited from NIPRISAN with no serious adverse effect. About 80% of the subjects did not experience any crisis during the study (12 months). The subjects experienced significant reduction in hospital admission while attendance at school profoundly increased. Furthermore, there was no evidence of kidney or liver damage. NIPRISAN has been patented, licensed to an American company, registered and being manufactured at Abuja for global market.
http://www.uneca.org/sciencewithafrica/content/swa_book_of_abstacts-en.pdf
NICOSAN / NIPRISAN
Post a Comment