 Happy New Year 2008
Happy New Year 2008For those who will be sitting MRCP Part 1 and 2 in 2008, good luck and YOU CAN DO IT!!
Make a resolution today and hope 2008 will be a happy year for everyone!!
Happy New Year 2008



 Unilateral leg swelling
Unilateral leg swelling

 Normal. Inspiratory limb of loop is symmetric and convex. Expiratory limb is linear. Flow rates at the midpoint of the inspiratory and expiratory capacity are often measured. Maximal inspiratory flow at 50% of forced vital capacity (MIF 50% FVC) is greater than maximal expiratory flow at 50% FVC (MEF 50%FVC) because dynamic compression of the air-ways occurs during exhalation.
Normal. Inspiratory limb of loop is symmetric and convex. Expiratory limb is linear. Flow rates at the midpoint of the inspiratory and expiratory capacity are often measured. Maximal inspiratory flow at 50% of forced vital capacity (MIF 50% FVC) is greater than maximal expiratory flow at 50% FVC (MEF 50%FVC) because dynamic compression of the air-ways occurs during exhalation.
 The loop is narrowed because of diminished lung volumes, but the shape is generally the same as in nor-mal volume. Flow rates are greater than normal at comparable lung volumes because the increased elastic recoil of lungs holds the airways open.
The loop is narrowed because of diminished lung volumes, but the shape is generally the same as in nor-mal volume. Flow rates are greater than normal at comparable lung volumes because the increased elastic recoil of lungs holds the airways open.



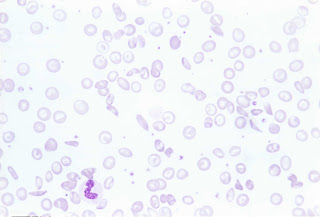 ( Blood film of sickle cell, polychromasia and target cell)
( Blood film of sickle cell, polychromasia and target cell)
By far, I think this the most popular blood film in MRCP. Remember that patients with sickle cell may present with bone pain ( due to bone necrosis), osteomyelitis, leg ulcers or even iron overload. Remember that it is one of the important causes of chronic haemolysis anaemia, therefore, you might find pallor with jaundice in patients with Sickle Cell Disease. However, remember that you may not find splenomegaly ( although you anticipate splenomegaly in patients with chronic haemolysis) because there is a possibility of splenic infarct!!
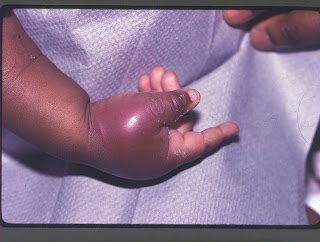 ( Patient presents with painful bony infarction)
( Patient presents with painful bony infarction)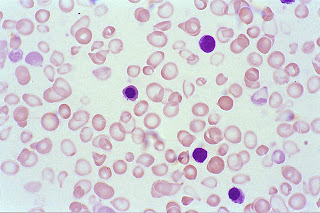 ( Blood film showing hypochromic, microcyctic red cells)
( Blood film showing hypochromic, microcyctic red cells)


 Note: Always remember that shortened PR interval occurs in WPW syndrome!
Note: Always remember that shortened PR interval occurs in WPW syndrome! b) Mobitz type 2- For this heart block, AV block the PR intervals are constant until a nonconducted P wave occurs. ( as below ECG)
b) Mobitz type 2- For this heart block, AV block the PR intervals are constant until a nonconducted P wave occurs. ( as below ECG) Third degree heart block
Third degree heart block
 Basophilic stippling of RBCs is seen in lead poisoining, thalassemia and other dyserythropoetic anaemias
Basophilic stippling of RBCs is seen in lead poisoining, thalassemia and other dyserythropoetic anaemias



A COMPLETE third nerve plasy ( Above patient - right third nerve palsy) should have:
i) Dilated pupil (mydriasis)
ii) Ptosis
iii) Deviation of eye laterally and downward ( due to unopposed actions of lateral rectus and superior oblique)



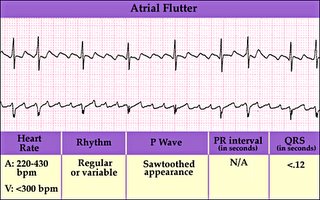
Always described as “ Saw-Tooth” ECG in medical textbook. The atrial activity is usually between 250-350 beats /min and there is sually 2:1 or 3:1 block. Causes for atrial flutter are similar to atrial fibrillation as well as the management.
3) Ventricular tachycardia

Defined as three or more successive ventricular extrasystoles at a rate more than 120/min. Remember than VT has a wide QRS complex. Causes of VT include
a) Ischaemia to the heart
b) Hypo-or hyperkl\alaemia
c) Long QT interval ( a very popular question in MRCP, I will cover this in depth in my future post)
d) Cardiomyopathies
4) Torsades des pointes

Actually it is a type of ventricular tachycardia with a varying axis. It often happens after heart attack but can be due to drugs and other causes of prolonged QT interval.
5) Ventricular fibrillation
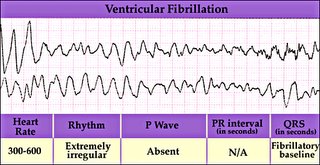
This rhythm needs immediate cardioversion. Usually happens after a hear attack
Important Tips for MRCP,
It is often difficult to differentiate an SVT with abberant ventricular conduction from VT ( both also have wide QRS complexes), however always remember in clinical practice, always assume VT if you are in doubt and treat accordingly because VT is commoner and life threatening. However, following features suggest SVT with abberant blocks,
1) No fusion or capture beats
2) Presence of P waves associated with ORS
3) Classical RBBB and LBBB ORS morphology
4) ORS <0.14s
5) Same QRS morphology as in sinus rhythm
6) Normal axis

Nerve I, Olfactory nerve- just remember that it is for smell
Nerve II ( Optic) and Nerve III ( Occulomotor) are important nerves to remember,
There are a few common questions asked in MRCP about these two nerves,
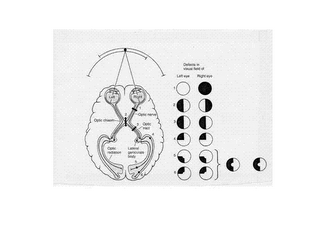
a) Remember that Optic nerve is for vision and you must always remember the visual fields , it is important in your MRCP Part1,2 as well as in MRCP PACES
b) Remember your afferent fiber for your pupillary reflex is your optic nerve and your efferent fiber is Occulomotor ( therefore occulomotor nerve is a parasympathetic fiber)
c) Remember that other components of Occulomotor nerve ( besides its parasympathetic function in constricting pupil) are motor components supplying all extraocular muscles except lateral rectus and superior oblique. It also supplies levator palpebrae superoris.
Therefore, a complete third nerve palsy gives,
i) Dilated pupil (mydriasis)
ii) Ptosis
iii) Deviation of eye laterally and downward ( due to unopposed actions of lateral rectus and superior oblique)
SO…….., one very,very important formula to remember in eye movement is (LR6SO4)3, lateral rectus is supplied by sixth nerve (abducent nerve) and superior oblique is supplied by fourth nerve (Trochlear nerve) and others are supplied by third nerve ( Occulomotor)
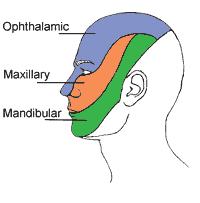
You will be surprised that we have learned 5 nerves out of first six cranial nerves, the fifth cranial nerve is trigeminal nerve, just remember that its sensory component supplying the facial sensory dermatomes ( One popular question in MRCP is they will show a patient with shingles over the face and you are expected to know what sensory component of trigeminal nerve is involved!)
 (A-splinter haemorrhage, B-Conjunctival petechiae, C-Osler's node, D-Janeway's Lesion)
(A-splinter haemorrhage, B-Conjunctival petechiae, C-Osler's node, D-Janeway's Lesion)
( There is a criteria for you to diagnose Infective Endocarditis known as Durack’s criteria, you do not need to know about the details, however, remember that the two major criteria are positive isolation of organisms from blood culture and evidence of endocardial involvement on ECHO)
Investigations
Full blood count- raised TWC and anemia ( normocystic, normochromic), raised ESR
Haematuria may be present in 50% of cases
Blood culture ( remember that you may need CO2 culture for fastidious HACEK organisms-Haemophilus, Actinobacillus,Cardiobacterium,Eikenella and Kingella)
Complications
Mainly due to septic emboli- the emboli can go to brain, spleen, liver, lung leading to abscess formation. In the heart, infective endocarditis can cause valvular failure, heart block and prosthesis failure!
Treatment
Prolonged IV antibiotics ( up to 4-6 weeks) , usually combination of IV penicillin + gentamycin.
Surgery is indicated if development of fungal endocarditis, valve dehiscence, heart block, valve ring abscesses, failure of medical treatment!
Tips for MRCP
1) Remember patients with what valvular heart lesions need antibiotics prophylaxis before invasive procedures. Click here to find out more!
2) Remember what do you mean by invasive procedures, click here to learn more!

Here is why I would like you to consider joining:
1. AGLOCO pays you, as an Internet user, your fair share of the value created while you surf.
2. The AGLOCO's free software puts you in control of what arrives on your screen and what data you allow outsiders to collect.
3. AGLOCO is a 100% Member owned company which rewards the Members who help build the company. It never costs anything to be a Member AGLOCO is only four weeks old and it has already signed up tens of thousands of Members and has created enormous Internet 'buzz' (over 700,000 pages in Google's search talk about AGLOCO).

AGLOCO is not a 'get rich' quick scheme. Every additional Member raises the value of all the Members, so we all get more if you join.
Learn more abouth this program at http://www.investing-tip.com/makemoney.html
It is free to join and Membership never costs anything. Click here to read more and sign up now. CLICK HERE NOW TO JOIN!
Thanks
PassMRCP
