Anatomy was a hell for me when I was a medical student. There is no trick to be good in anatomy except you have a good memory. Luckily, there are not so many questions about anatomy being asked in MRCP Part 1. I will try to cover basic anatomy in a few posts and I hope the information provided in this blog will be useful for you to answer your MRCP questions.
OK, today I will try to cover the first 6 cranial nerves today and I will try to give you a few popular questions in MRCP.
Refresh your memory first and remember all 12 cranial nerves ,

Nerve I, Olfactory nerve- just remember that it is for smell
Nerve II ( Optic) and Nerve III ( Occulomotor) are important nerves to remember,
There are a few common questions asked in MRCP about these two nerves,
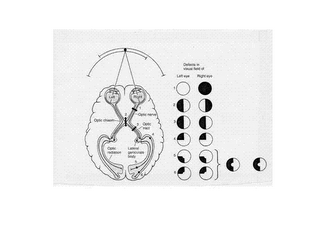
a) Remember that Optic nerve is for vision and you must always remember the visual fields , it is important in your MRCP Part1,2 as well as in MRCP PACES
b) Remember your afferent fiber for your pupillary reflex is your optic nerve and your efferent fiber is Occulomotor ( therefore occulomotor nerve is a parasympathetic fiber)
c) Remember that other components of Occulomotor nerve ( besides its parasympathetic function in constricting pupil) are motor components supplying all extraocular muscles except lateral rectus and superior oblique. It also supplies levator palpebrae superoris.
Therefore, a complete third nerve palsy gives,
i) Dilated pupil (mydriasis)
ii) Ptosis
iii) Deviation of eye laterally and downward ( due to unopposed actions of lateral rectus and superior oblique)
SO…….., one very,very important formula to remember in eye movement is (LR6SO4)3, lateral rectus is supplied by sixth nerve (abducent nerve) and superior oblique is supplied by fourth nerve (Trochlear nerve) and others are supplied by third nerve ( Occulomotor)
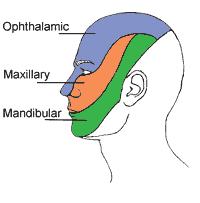
You will be surprised that we have learned 5 nerves out of first six cranial nerves, the fifth cranial nerve is trigeminal nerve, just remember that its sensory component supplying the facial sensory dermatomes ( One popular question in MRCP is they will show a patient with shingles over the face and you are expected to know what sensory component of trigeminal nerve is involved!)
 (A-splinter haemorrhage, B-Conjunctival petechiae, C-Osler's node, D-Janeway's Lesion)
(A-splinter haemorrhage, B-Conjunctival petechiae, C-Osler's node, D-Janeway's Lesion)

