
Although I will think that thrombocytopenia is not such a common case in MRCP, it is certainly a very common scenario in clinical practice.
The best way to think about high/low level in clinical medicine is the remember logically how a subtance/ product is being produced and destroyed in the normal physiology.
Therefore, low thrombocytopenia can be due to 2 main causes- reduced production from the bone marrow or increased destruction in the periphery.
I will talk about HIT ( Heparin Induced Thrombocytopenia) today in this post.
If you ask who is prone to get HIT, then I think is the group of patients who is being exposed to heparin almost everday. Yes, you are right, these patients are End stage renal failure patients who are on regular haemodialysis.
There are 2 types of HIT- early and late stage HIT. Type 1 HIT refers to condition of thrombocytopenia developing 1-2 days after heparin usage. It is a non immune condition due to direct effect of heparin on platelet. It is usually self-limiting and the platelet count usually normalizes after continued heaprin usage.
For type 2 HIT, it is an immune condition that happens later, usually 4-10 days after usage and it is life-threatening. The only option you have is to stop heparin usage.

 There are a few important fact to remember for MRCP,
There are a few important fact to remember for MRCP,






 Unilateral leg swelling
Unilateral leg swelling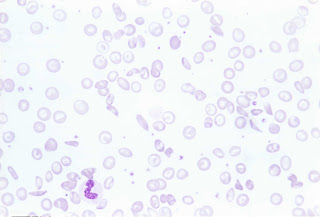 ( Blood film of sickle cell, polychromasia and target cell)
( Blood film of sickle cell, polychromasia and target cell)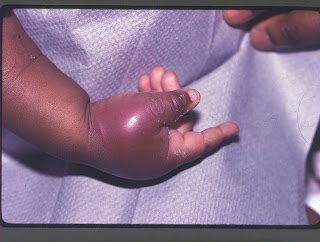 ( Patient presents with painful bony infarction)
( Patient presents with painful bony infarction)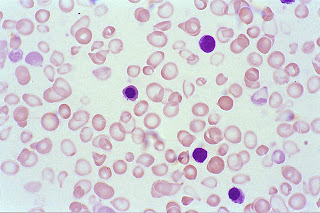 ( Blood film showing hypochromic, microcyctic red cells)
( Blood film showing hypochromic, microcyctic red cells)


