CYCLOSPORIN
Today, we want to learn another drug that is commonly asked in MRCP. Cyclosporin is a fungal peptide( discovered in 1972) with potent immunosuppressive activity. It acts to block transcription of mRNA for IL-2 and other proinflammatory cytokines, thereby inhibiting T cell proliferation.
Indications of Cyclosporin
Mainly for immunsuppresion after organ transplant
Rheumatoid arthritis
Auto-immune disease such as SLE
Psoriasis
Inflammatory Bowel Disease
Common side effects
Hypertension and diabetes
Excessive hair growth
Tremor
Nephrotoxicity
Hepatotoxicity
Gum hypertrophy
Electrolyte imbalance
Common interaction
It is mainly excreted by the liver in bile (about 90%), therefore cyclosporin level is increased by drugs which compete with c-p450 liver enzymes ( remember about erythromycin and cimetidine). For doctors, remember that grapefruit juice increases the level of cyclosporine.
Sunday, July 30, 2006
Thursday, July 27, 2006
ATRIAL FIBRILLATION
Atrial Fibrillation in MRCP
Questions about atrial fibrillation are commonly asked in MRCP, there are a few important points to take note in order for you to be able to answer all cardiology questions about AF.
ECG for AF
 ECG with AF is above and below is an ECG with sinus rhythm
ECG with AF is above and below is an ECG with sinus rhythm
Remember that AF is a supraventricular tachyarrhythmia characterized by an ECG with absent P waves.
Causes for AF
Ischaemic heart disease
Thyrotoxicosis
Chronic rheumatic heart disease especially mitral stenosis
Post surgery
Chronic lung disease
Alcohol intoxication
Atrial septal defect
Types of Atrial Fibrillation
Remember that patients can have permanent AF ( it is unlikely the rhythm be reverted to sinus rhythm, you can anticipate this if patient has AF longer than 1 year, ECHO shows dilated left atrium ( >5cm)and patient is older. Patient may also have paroxysmal AF where there is possibility that the rhythm can be reverted to sinus rhythm.
Cardioversion
Cardioversion of AF to sinus rhythm can be done either electrically or pharmacologically,
However, remember that for elective cardioversion ( electrical or pharmacological), anticoagulate patients with AF >48 hours with warfarin 3-4 weeks before and after cardioversion.
Electrical cardioversion can be performed with synchronized DC shock of 50 till 100 J
Drugs used for Pharmacological Cardioversion
These drugs include amiodarone, flecanide, ibutilide, dofetilide, propafenone and quinidine. ( Learn more about amiodarone and flecanide)
Acute Management of Fast AF
Remember the principles below,
a) Sustain haemodynamic stability
b) Control ventricular rhythm
c) Anticoagulation
d) Find the underlying cause
e) Long term cardioversion ( rhythm control) or rate control
If a patient is admitted for fast atrial fibrillation, first thing to assess is patient’s haemodynamic stability, if patient’s blood pressure is unstable , urgent DC shock is needed. However, if the patient is stable and has fast AF, try to control the ventricular rhythm. Two common drugs are used, beta-blocker or digoxin, digoxin is preferred if patient has heart failure.
After the patient is stable, try to find the underlying cause for the problem. If you think patient has permanent AF or paroxysmal AF and planned for cardioversion, discuss anticoagulation ( warfarin) with the patient. You may just want to have rate control if you think patient is unlikely to be reverted back to sinus rhythm!
MRCP Questions
1)The following are recognised causes of atrial fibrillation EXCEPT
A anxiety
B hyperthyroidism
C atrial septal defect
D alcohol abuse
E COAD
ANSWER: A
2)A patient presenting with atrial fibrillation who has reverted to sinus rhythm is more likely to remain in sinus rhythm in the following circumstances:
A age >75 years old
B been commenced on warfarin
C left atrium size > 6 cm on ECHO
D short history on AF
E a ventricular rate on presentation of 130 bpm
ANSWER: D
3)Causes of atrial fibrillation include:
A Aortic stenosis
B Maladie de Roger VSD
C anxiety
D recent MI
E complete heart block
ANSWER: D
4) A 70 year-old lady presents with sudden breathlessness and chest discomfort. On examination, she was observed to have an irregular heart beat with rate of 140 bpm, BP 122/74 and normal heart sounds. On auscultation of the chest, Fine basal crepitations are heard. An ECG confirms fast. She is anticoagulated with heparin and given diuretics. Her heart rate remains rapid. What is the most appropriate management of the lady's AF?
1 ) Cardioversion.
2 ) IV amiodarone.
3 ) IV betablocker.
4 ) IV digoxin.
5 ) Oral quinidine therapy.
ANSWER: 4
5)A 70-year-old woman has a history of dyspnoea and palpitations for six months. An ECG at that time showed atrial fibrillation. She was given digoxin, diuretics and aspirin. She now presents with two short-lived episodes of altered sensation in the left face, left arm and leg. There is poor coordination of the left hand. ECHO was normal as was a CT head scan.
What is the most appropriate next step in management?
1 ) anticoagulation
2 ) carotid endarterectomy
3 ) clopidogrel
4 ) corticosteroid treatment
5 ) no action
ANSWER: 1
6)A 48 year-old MAN with atrial fibrillation is admitted for DC cardioversion.He is reverted to sinus rhythm. Which one of the following drugs would be most likely to maintain sinus rhythm following this procedure?
1 ) amiodarone
2 ) digoxin
3 ) heparin
4 ) sotalol
5 ) verapamil
ANSWER: 1
7)A 50-year-old politician presented with a strange fluttering sensation in his chest, but no chest pain. The symptoms had lasted 24 hours. An ECG revealed atrial fibrillation with a ventricular rate of 130 beats per minute.
Which one of the following drugs is most likely to restore sinus rhythm?
1 ) Adenosine
2 ) Bisoprolol
3 ) Digoxin
4 ) Flecainide
5 ) Verapamil
ANSWER: 4
8)The risk of embolic stroke with atrial fibrillation is increased in: EXCEPT
A Left ventricular ejection fraction of 60%.
B Diabetes mellitus.
C Controlled hypertension.
D Age greater than 75 years.
E Rheumatic mitral valve disease.
ANSWER: A
Questions about atrial fibrillation are commonly asked in MRCP, there are a few important points to take note in order for you to be able to answer all cardiology questions about AF.
ECG for AF
 ECG with AF is above and below is an ECG with sinus rhythm
ECG with AF is above and below is an ECG with sinus rhythmRemember that AF is a supraventricular tachyarrhythmia characterized by an ECG with absent P waves.
Causes for AF
Ischaemic heart disease
Thyrotoxicosis
Chronic rheumatic heart disease especially mitral stenosis
Post surgery
Chronic lung disease
Alcohol intoxication
Atrial septal defect
Types of Atrial Fibrillation
Remember that patients can have permanent AF ( it is unlikely the rhythm be reverted to sinus rhythm, you can anticipate this if patient has AF longer than 1 year, ECHO shows dilated left atrium ( >5cm)and patient is older. Patient may also have paroxysmal AF where there is possibility that the rhythm can be reverted to sinus rhythm.
Cardioversion
Cardioversion of AF to sinus rhythm can be done either electrically or pharmacologically,
However, remember that for elective cardioversion ( electrical or pharmacological), anticoagulate patients with AF >48 hours with warfarin 3-4 weeks before and after cardioversion.
Electrical cardioversion can be performed with synchronized DC shock of 50 till 100 J
Drugs used for Pharmacological Cardioversion
These drugs include amiodarone, flecanide, ibutilide, dofetilide, propafenone and quinidine. ( Learn more about amiodarone and flecanide)
Acute Management of Fast AF
Remember the principles below,
a) Sustain haemodynamic stability
b) Control ventricular rhythm
c) Anticoagulation
d) Find the underlying cause
e) Long term cardioversion ( rhythm control) or rate control
If a patient is admitted for fast atrial fibrillation, first thing to assess is patient’s haemodynamic stability, if patient’s blood pressure is unstable , urgent DC shock is needed. However, if the patient is stable and has fast AF, try to control the ventricular rhythm. Two common drugs are used, beta-blocker or digoxin, digoxin is preferred if patient has heart failure.
After the patient is stable, try to find the underlying cause for the problem. If you think patient has permanent AF or paroxysmal AF and planned for cardioversion, discuss anticoagulation ( warfarin) with the patient. You may just want to have rate control if you think patient is unlikely to be reverted back to sinus rhythm!
MRCP Questions
1)The following are recognised causes of atrial fibrillation EXCEPT
A anxiety
B hyperthyroidism
C atrial septal defect
D alcohol abuse
E COAD
ANSWER: A
2)A patient presenting with atrial fibrillation who has reverted to sinus rhythm is more likely to remain in sinus rhythm in the following circumstances:
A age >75 years old
B been commenced on warfarin
C left atrium size > 6 cm on ECHO
D short history on AF
E a ventricular rate on presentation of 130 bpm
ANSWER: D
3)Causes of atrial fibrillation include:
A Aortic stenosis
B Maladie de Roger VSD
C anxiety
D recent MI
E complete heart block
ANSWER: D
4) A 70 year-old lady presents with sudden breathlessness and chest discomfort. On examination, she was observed to have an irregular heart beat with rate of 140 bpm, BP 122/74 and normal heart sounds. On auscultation of the chest, Fine basal crepitations are heard. An ECG confirms fast. She is anticoagulated with heparin and given diuretics. Her heart rate remains rapid. What is the most appropriate management of the lady's AF?
1 ) Cardioversion.
2 ) IV amiodarone.
3 ) IV betablocker.
4 ) IV digoxin.
5 ) Oral quinidine therapy.
ANSWER: 4
5)A 70-year-old woman has a history of dyspnoea and palpitations for six months. An ECG at that time showed atrial fibrillation. She was given digoxin, diuretics and aspirin. She now presents with two short-lived episodes of altered sensation in the left face, left arm and leg. There is poor coordination of the left hand. ECHO was normal as was a CT head scan.
What is the most appropriate next step in management?
1 ) anticoagulation
2 ) carotid endarterectomy
3 ) clopidogrel
4 ) corticosteroid treatment
5 ) no action
ANSWER: 1
6)A 48 year-old MAN with atrial fibrillation is admitted for DC cardioversion.He is reverted to sinus rhythm. Which one of the following drugs would be most likely to maintain sinus rhythm following this procedure?
1 ) amiodarone
2 ) digoxin
3 ) heparin
4 ) sotalol
5 ) verapamil
ANSWER: 1
7)A 50-year-old politician presented with a strange fluttering sensation in his chest, but no chest pain. The symptoms had lasted 24 hours. An ECG revealed atrial fibrillation with a ventricular rate of 130 beats per minute.
Which one of the following drugs is most likely to restore sinus rhythm?
1 ) Adenosine
2 ) Bisoprolol
3 ) Digoxin
4 ) Flecainide
5 ) Verapamil
ANSWER: 4
8)The risk of embolic stroke with atrial fibrillation is increased in: EXCEPT
A Left ventricular ejection fraction of 60%.
B Diabetes mellitus.
C Controlled hypertension.
D Age greater than 75 years.
E Rheumatic mitral valve disease.
ANSWER: A
Tuesday, July 25, 2006
HEREDITARY HAEMOCHROMATOSIS
HEREDITARY HAEMOCHROMATOSIS (HH)
Today, I am going to talk about an important disease in gastroenterology. This disease is commonly asked in MRCP and popular questions being asked in MRCP Part 1 as well as Part 2 are as follow,
a) data interpretation for iron profile of a patient,
b) Presentations of hereditary haemochromatosis, usually a patient with non- specific joint pain,
c) Complications of HH,
d) HLA A3 association with the disease
Hereditary haemochhromatosis is a condition where there is abnormal high absorption of iron by the gut mucosa leading to iron overload in the body. It is another common cause of chronic liver disease in young age population besides Wilson’s disease. Remember that hereditary haemochromatosis is the commonest cause of iron overload in Western countries whereas in developing countries and Middle East, multiple frequent transfusions is the major cause of iron overload especially among patients with Thalassemia.
Data Interpretation For Hereditary Haemochromatosis
Features
Total iron increased
Ferritin increased
Fasting transferring saturation increased
Remember that due to iron overload in all organs especially endocrine organs such as pituitary, gonads, pancreas and also liver, cartilage, joints and etc this eventually leads to development of Diabetes mellitus, low testosterone and possibility of low libido and infertility.
Common presentations of Hereditary Haemochromatosis
Due to above reasons ( iron overload), patient may present with
- unspecific joint pain,
- chronic liver disease ( liver cirrhosis) and lead to liver cancer
- loss of libido and infertility
- DM
Complications of HH
Liver cirrhosis
Cardiomyopathy ( due to iron overload over cardiac muscle)
Treatment of HH
Recurrent phlebotomy, avoid Vit C ( can increase iron absorption) and alcohol.
Today, I am going to talk about an important disease in gastroenterology. This disease is commonly asked in MRCP and popular questions being asked in MRCP Part 1 as well as Part 2 are as follow,
a) data interpretation for iron profile of a patient,
b) Presentations of hereditary haemochromatosis, usually a patient with non- specific joint pain,
c) Complications of HH,
d) HLA A3 association with the disease
Hereditary haemochhromatosis is a condition where there is abnormal high absorption of iron by the gut mucosa leading to iron overload in the body. It is another common cause of chronic liver disease in young age population besides Wilson’s disease. Remember that hereditary haemochromatosis is the commonest cause of iron overload in Western countries whereas in developing countries and Middle East, multiple frequent transfusions is the major cause of iron overload especially among patients with Thalassemia.
Data Interpretation For Hereditary Haemochromatosis
Features
Total iron increased
Ferritin increased
Fasting transferring saturation increased
Remember that due to iron overload in all organs especially endocrine organs such as pituitary, gonads, pancreas and also liver, cartilage, joints and etc this eventually leads to development of Diabetes mellitus, low testosterone and possibility of low libido and infertility.
Common presentations of Hereditary Haemochromatosis
Due to above reasons ( iron overload), patient may present with
- unspecific joint pain,
- chronic liver disease ( liver cirrhosis) and lead to liver cancer
- loss of libido and infertility
- DM
Complications of HH
Liver cirrhosis
Cardiomyopathy ( due to iron overload over cardiac muscle)
Treatment of HH
Recurrent phlebotomy, avoid Vit C ( can increase iron absorption) and alcohol.
Monday, July 24, 2006
RHEUMATIC FEVER
RHEUMATIC FEVER
Another popular topic in MRCP cardiology, common questions being asked in MRCP part 1 as well as part 2 are as follow,
a) Duckett Jones criteria to diagnose rheumatic fever,
b) Relationship between rheumatic fever and streptococcal infection,
c) Common presentations of rheumatic fever
d) Acute treatment for rheumatic fever
Why is rheumatic fever so important in MRCP? I think it is because the major cause of valvular heart diseases in developing countries is still chronic rheumatic disease.
DUCKETT JONES CRITERIA
The mnemonic to remember SPEC2 + WAFER2
Major Criteria
Subcutaneous nodule
Polyarthritis-described as migratory
Erythema marginatum
Carditis – pancarditis, usually in acute setting, no murmur can be heard, but there is possibility of mid-diastolic murmur ( Carey Coombes murmur)
Chorea- Sydenham’s chorea
Minor Criteria
White cells- raised ( leucocytosis)
Arthragia
Fever
ESR- raised or CRP
Rheumatic fever ( previous history)
PR interval prolonged
Diagnosis: Recent Streptococcal infection ( raised ASOT) + 2 majors or 1 major and 2 minors.
Streptococcal Infection and Rheumatic fever
Rheumatic fever usually occurs 3 weeks after Group A streptococcal infection.
Acute Treatment
Penicillin + aspirin ( high dose) and +/- steroid ( prednisolone)
Another popular topic in MRCP cardiology, common questions being asked in MRCP part 1 as well as part 2 are as follow,
a) Duckett Jones criteria to diagnose rheumatic fever,
b) Relationship between rheumatic fever and streptococcal infection,
c) Common presentations of rheumatic fever
d) Acute treatment for rheumatic fever
Why is rheumatic fever so important in MRCP? I think it is because the major cause of valvular heart diseases in developing countries is still chronic rheumatic disease.
DUCKETT JONES CRITERIA
The mnemonic to remember SPEC2 + WAFER2
Major Criteria
Subcutaneous nodule
Polyarthritis-described as migratory
Erythema marginatum
Carditis – pancarditis, usually in acute setting, no murmur can be heard, but there is possibility of mid-diastolic murmur ( Carey Coombes murmur)
Chorea- Sydenham’s chorea
Minor Criteria
White cells- raised ( leucocytosis)
Arthragia
Fever
ESR- raised or CRP
Rheumatic fever ( previous history)
PR interval prolonged
Diagnosis: Recent Streptococcal infection ( raised ASOT) + 2 majors or 1 major and 2 minors.
Streptococcal Infection and Rheumatic fever
Rheumatic fever usually occurs 3 weeks after Group A streptococcal infection.
Acute Treatment
Penicillin + aspirin ( high dose) and +/- steroid ( prednisolone)
Systemic lupus erythematosis (SLE)
Systemic lupus erythematosis (SLE)
As I mentioned in my previous post ( 100 common questions in MRCP), SLE is always a popular question in either MRCP Part 1 or 2. There are a few typical and popular questions about SLE in MRCP, these include,
a) Photo-based question, usually a patient with malar rash would be shown in exam. Find a photo of SLE here, click www.passpaces.com/MRCP/issue1.html
b) The criteria to diagnose SLE, remember about American Rheumatic Association (ARA) criteria,
c) Common presentations of SLE and its complications
d) Drugs used in SLE and its side effects
e) Drug-induced SLE
ARA criteria
The mnemonic to remember HAI, MOPD ‘N’ RAS
Haematological involvement- can be thrombocytopenia, neutropenia , haemolysis or even pancytopenia.
Antinuclear antibody- seen in more than 90% of patients
Immunological disorder- anti-DNA, positive syphilis test, low C3,C4
Malar rash
Oral ulcers
Photosensitive rash
Discoid rash
Neurological involvement-pyschosis, fit
Renal involvement- lupus nephritis, protenuria
Arthritis- joint involvement
Serositis –pleuritis,pericarditis, endocarditis (Libman-Sacs)
To diagnose SLE, any four out of 11 criteria above!
Common drugs that cause drug-induced lupus are procainamide, isoniazid and hydralazine (PIH)
To diagnose drug-induced lupus, remember that
1) There will be sparing of renal and central nervous system
2) Anti-histone antibodies will be positive
Common presentations of SLE
Almost any thing under the sun, however, in MRCP, they would usually give you a case who is a young lady presents with unexplained fever and you notice that almost every organ is involved, investigations may show low white cell +/- platelets, renal involvement ( presence of RBC or protein) etc. Remember, 99% is a female patient!!
Common drugs used in SLE
I would cover this in my serial of popular drugs in MRCP in my coming posts. These drugs include prednisolone, azathioprine, hydroxychloroquine, cyclophosphamide and cyclosporin. ( immunosuppresants)
As I mentioned in my previous post ( 100 common questions in MRCP), SLE is always a popular question in either MRCP Part 1 or 2. There are a few typical and popular questions about SLE in MRCP, these include,
a) Photo-based question, usually a patient with malar rash would be shown in exam. Find a photo of SLE here, click www.passpaces.com/MRCP/issue1.html
b) The criteria to diagnose SLE, remember about American Rheumatic Association (ARA) criteria,
c) Common presentations of SLE and its complications
d) Drugs used in SLE and its side effects
e) Drug-induced SLE
ARA criteria
The mnemonic to remember HAI, MOPD ‘N’ RAS
Haematological involvement- can be thrombocytopenia, neutropenia , haemolysis or even pancytopenia.
Antinuclear antibody- seen in more than 90% of patients
Immunological disorder- anti-DNA, positive syphilis test, low C3,C4
Malar rash
Oral ulcers
Photosensitive rash
Discoid rash
Neurological involvement-pyschosis, fit
Renal involvement- lupus nephritis, protenuria
Arthritis- joint involvement
Serositis –pleuritis,pericarditis, endocarditis (Libman-Sacs)
To diagnose SLE, any four out of 11 criteria above!
Common drugs that cause drug-induced lupus are procainamide, isoniazid and hydralazine (PIH)
To diagnose drug-induced lupus, remember that
1) There will be sparing of renal and central nervous system
2) Anti-histone antibodies will be positive
Common presentations of SLE
Almost any thing under the sun, however, in MRCP, they would usually give you a case who is a young lady presents with unexplained fever and you notice that almost every organ is involved, investigations may show low white cell +/- platelets, renal involvement ( presence of RBC or protein) etc. Remember, 99% is a female patient!!
Common drugs used in SLE
I would cover this in my serial of popular drugs in MRCP in my coming posts. These drugs include prednisolone, azathioprine, hydroxychloroquine, cyclophosphamide and cyclosporin. ( immunosuppresants)
Friday, July 21, 2006
MRCP Part 2 Questions
MRCP PART 2 QUESTIONS
Hope you find these questions useful, I will be uploading questions regularly,
1)72 year old female was admitted with a deteriorating dyspnoea and fever which had deteriorated over the preceding three days. Prior to this admission she had been well having returned one week ago from an Asian holiday with her husband. She is a smoker of 5 cigarettes per day. On examination she was suntanned, slightly confused with saturations of 92% on air. She had a pyrexia of 40oC, a pulse of 118 bpm and a blood pressure of 118/90 mmHg. Auscultation of the chest revealed left basal crackles only. The following detail her investigations:Haemoglobin 14.3 g/dlWhite cell count 8.2 x109/lPlatelets 320 x109/lSerum Sodium 123 mmol/lSerum Potassium 3.6 mmol/lUrea 4.2 mmol/lPlasma Glucose 10.9 mmol/lUrine sodium concentration 35 mmol/lArterial blood gas analysis:pH 7.36pCO2 38 mmHg pO2 80 mmHgStandard bicarbonate 30 mmol/lWhich of the following tests would be most useful in providing diagnostic information?
1 ) Blood culture
2 ) Serum antibody tests
3 ) Short synacthen test
4 ) Sputum culture
5 ) Urine antigen test
ANSWER: 5
2)A 22 year old male is referred by his General practitioner due to problems related to his sex life. He has recently entered into his first sexual relationship but is worried by his poor sexual development. He is aware of a paucity of pubic hair and he has been embarrassed about his gonadal development. He started to shave at the age of 18 but shaves only twice weekly. He is quite fit and active and works as a labourer on a building site. He takes no medication and drinks 20 units of alcohol weekly, mostly on weekends. He has one younger brother. Examination reveals a phenotypically normal male, who is tall but lean with a BMI of 21.2 kg/m2. He has little beard growth, fine skin, a paucity of body hair and scanty pubic hair. His penile length is approximately 6 cm with testicular volumes of approximately 6-7 mls bilaterally (Normal 10-15 mls). Cardiovascular, respiratory and abdominal examination are all normal. Fundal examination is normal and he has normal visual fields.
His investigations are as follows:
Plasma testosterone concentration 6.2 nmol/l (10 - 30)
LH 20.2 mU/l (2-10)
FSH 22.2 mU/l (2-10)
Prolactin 433 mU/l (50-500)
free T4 12.6 nmol/l (9-23)
TSH 2.3 mU/l (0.5-4.5)
What are the chances of his brother developing this disorder?
1 ) <1%
2 ) 25%
3 ) 50%
4 ) 75%
5 ) 100%
ANSWER: 1
3)A 69 year-old lady presents to you complaining of being non-specifically unwell over the last month. She is stiff especially in the mornings and has difficulty lifting her hands to comb her hair. Her arms and shoulders ache constantly and she has jaw pain when chewing. She has lost 4kg in weight and has a persistent headache. She smokes 10 cigarettes a day and consumes 10 units of alcohol a week.On examination, temperature is 38°C, pulse 84 beats/min and BP 125/80. Apart from reduced power in the proximal muscles of her arms and legs, the rest of the examination is unremarkable.Investigations:Hb 9.9 g/dl
WCC 13.9 x 109/l
Platelets 400 x 109/l
Plasma sodium 139 mmol/l
Plasma potassium 4.7 mmol/l
Plasma urea 5.0 mmol/l
Plasma creatinine 109 µmol/l
Plasma glucose 5.9 mmol/l
Bilirubin 15 µmol/l (normal range 3-17 µmol/l)
Plasma alkaline phosphatase 390 iu/l (normal range 30-300 iu/l)
Plasma aspartate transaminase 65 iu/l (normal range 5-35 iu/l)
Plasma creatine kinase 150 iu/l (normal range 25-195 iu/l)
What is the most appropriate investigation to be performed next?
1 ) Anti-double stranded DNA antibodies
2 ) Erythrocyte sedimentation rate
3 ) Muscle biopsy
4 ) Plasma calcium
5 ) Thyroid function tests
ANSWER: 2
4)A 50 year old woman presents with dry eyes, a dry mouth, an erythematous rash and polyarthralgia. Investigations: ANA strongly positive (1:1600), anti-Ro/SSA antibodies strongly positive, rheumatoid factor positive, IgG markedly elevated at 45 g/l (normal - <15 g/l), IgM and IgA levels are normal and the kappa/lambda ratio is normal. What is the most likely diagnosis?
1 ) Hyperviscosity syndrome
2 ) Myeloma associated vasculitis
3 ) Primary Sjogren's Syndrome
4 ) Rheumatoid arthritis with secondary Sjogren's Syndrome
5 ) Systemic Lupus Erythematosus
ANSWER: 3
5)This lady presents with dysphagia, what is the diagnosis?
Find the photo at www.passpaces.com/MRCP/issue8.html
1 ) Dermatomyositis
2 ) Raynaud's phenomenon
3 ) Systemic sclerosis
4 ) Plummer-Vinson syndrome
5 ) Hyperthyroidism
ANSWER:3
6)This gentleman has pain over with his ankle and presents with fever

1 ) Neurofibromatosis
2 ) Tuberose sclerosis
3 ) von Hippel-Lindau syndrome
4 ) Multiple endocrine neoplasia type IIb
5 ) Gardner's syndrome
ANSWER 2
Hope you find these questions useful, I will be uploading questions regularly,
1)72 year old female was admitted with a deteriorating dyspnoea and fever which had deteriorated over the preceding three days. Prior to this admission she had been well having returned one week ago from an Asian holiday with her husband. She is a smoker of 5 cigarettes per day. On examination she was suntanned, slightly confused with saturations of 92% on air. She had a pyrexia of 40oC, a pulse of 118 bpm and a blood pressure of 118/90 mmHg. Auscultation of the chest revealed left basal crackles only. The following detail her investigations:Haemoglobin 14.3 g/dlWhite cell count 8.2 x109/lPlatelets 320 x109/lSerum Sodium 123 mmol/lSerum Potassium 3.6 mmol/lUrea 4.2 mmol/lPlasma Glucose 10.9 mmol/lUrine sodium concentration 35 mmol/lArterial blood gas analysis:pH 7.36pCO2 38 mmHg pO2 80 mmHgStandard bicarbonate 30 mmol/lWhich of the following tests would be most useful in providing diagnostic information?
1 ) Blood culture
2 ) Serum antibody tests
3 ) Short synacthen test
4 ) Sputum culture
5 ) Urine antigen test
ANSWER: 5
2)A 22 year old male is referred by his General practitioner due to problems related to his sex life. He has recently entered into his first sexual relationship but is worried by his poor sexual development. He is aware of a paucity of pubic hair and he has been embarrassed about his gonadal development. He started to shave at the age of 18 but shaves only twice weekly. He is quite fit and active and works as a labourer on a building site. He takes no medication and drinks 20 units of alcohol weekly, mostly on weekends. He has one younger brother. Examination reveals a phenotypically normal male, who is tall but lean with a BMI of 21.2 kg/m2. He has little beard growth, fine skin, a paucity of body hair and scanty pubic hair. His penile length is approximately 6 cm with testicular volumes of approximately 6-7 mls bilaterally (Normal 10-15 mls). Cardiovascular, respiratory and abdominal examination are all normal. Fundal examination is normal and he has normal visual fields.
His investigations are as follows:
Plasma testosterone concentration 6.2 nmol/l (10 - 30)
LH 20.2 mU/l (2-10)
FSH 22.2 mU/l (2-10)
Prolactin 433 mU/l (50-500)
free T4 12.6 nmol/l (9-23)
TSH 2.3 mU/l (0.5-4.5)
What are the chances of his brother developing this disorder?
1 ) <1%
2 ) 25%
3 ) 50%
4 ) 75%
5 ) 100%
ANSWER: 1
3)A 69 year-old lady presents to you complaining of being non-specifically unwell over the last month. She is stiff especially in the mornings and has difficulty lifting her hands to comb her hair. Her arms and shoulders ache constantly and she has jaw pain when chewing. She has lost 4kg in weight and has a persistent headache. She smokes 10 cigarettes a day and consumes 10 units of alcohol a week.On examination, temperature is 38°C, pulse 84 beats/min and BP 125/80. Apart from reduced power in the proximal muscles of her arms and legs, the rest of the examination is unremarkable.Investigations:Hb 9.9 g/dl
WCC 13.9 x 109/l
Platelets 400 x 109/l
Plasma sodium 139 mmol/l
Plasma potassium 4.7 mmol/l
Plasma urea 5.0 mmol/l
Plasma creatinine 109 µmol/l
Plasma glucose 5.9 mmol/l
Bilirubin 15 µmol/l (normal range 3-17 µmol/l)
Plasma alkaline phosphatase 390 iu/l (normal range 30-300 iu/l)
Plasma aspartate transaminase 65 iu/l (normal range 5-35 iu/l)
Plasma creatine kinase 150 iu/l (normal range 25-195 iu/l)
What is the most appropriate investigation to be performed next?
1 ) Anti-double stranded DNA antibodies
2 ) Erythrocyte sedimentation rate
3 ) Muscle biopsy
4 ) Plasma calcium
5 ) Thyroid function tests
ANSWER: 2
4)A 50 year old woman presents with dry eyes, a dry mouth, an erythematous rash and polyarthralgia. Investigations: ANA strongly positive (1:1600), anti-Ro/SSA antibodies strongly positive, rheumatoid factor positive, IgG markedly elevated at 45 g/l (normal - <15 g/l), IgM and IgA levels are normal and the kappa/lambda ratio is normal. What is the most likely diagnosis?
1 ) Hyperviscosity syndrome
2 ) Myeloma associated vasculitis
3 ) Primary Sjogren's Syndrome
4 ) Rheumatoid arthritis with secondary Sjogren's Syndrome
5 ) Systemic Lupus Erythematosus
ANSWER: 3
5)This lady presents with dysphagia, what is the diagnosis?
Find the photo at www.passpaces.com/MRCP/issue8.html
1 ) Dermatomyositis
{kind=link}
2 ) Raynaud's phenomenon
3 ) Systemic sclerosis
4 ) Plummer-Vinson syndrome
5 ) Hyperthyroidism
ANSWER:3
6)This gentleman has pain over with his ankle and presents with fever

What is the most likely synovial fluid finding?
1 ) Bipyramidal crystals that exhibit strong positive birefringence under polarised light
2 ) Gram positive cocci in clusters
3 ) Needle-shaped crystals that exhibit strong negative birefringence under polarised light
4 ) Rhomboid crystals that exhibit weak positive birefringence under polarised light
5 ) Small, non-birefringent crystals visible only under electron microscopy
ANSWER:3
7)This lady presents to A+E lower limbs pain, what is the likely diagnosis? 1 ) Secondary syphilis
1 ) Secondary syphilis
2 ) Cat scratch fever
3 ) Oral contraceptive pill
4 ) Sarcoidosis
5 ) Streptococcal infection
ANSWER: 5
8)A 24 year old male who works in a plastic factory presented with shortness of breath. He went for 2 weeks to Thailand and was completely well. He presented to the Accident & Emergency Unit after having used his Salbutamol inhaler 3 times. .The most likely diagnosis is?
1 ) Broncho pulmonary aspergillosis
2 ) Chemical pneumonitis
3 ) Extrinsic allergic alveolitis
4 ) Late onset asthma
5 ) Occupational asthma
ANSWER: 5
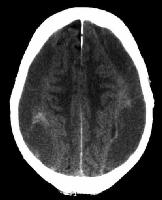
9)A 47-year-old man with HIV disease presents to hospital with a tonic-clonic seizure. He had initially presented six months previously with Pneumocystis carinii pneumonia with a CD4 T-lymphocyte count of 10 cells/mm3 and had subsequently started on highly active antiretroviral therapy. His most recent CD4 count, taken one month prior to his new presentation, was 50 cells/mm3. On examination he has no focal weakness, but both plantar responses are extensor. Fundoscopy is normal.A CT scan of his brain is shown.

1) AIDS related dementia
2 ) Brain abscess
3 ) Cerebral toxoplasmosis
4 ) Primary CNS lymphoma
5 ) Progressive multifocal leukoencephalopathy
ANSWER: 3
10)This 32 year-old gentleman presented with a grand mal seizure. CT scan of his head showed several small areas of periventricular calcification.

1 ) Neurofibromatosis
2 ) Tuberose sclerosis
3 ) von Hippel-Lindau syndrome
4 ) Multiple endocrine neoplasia type IIb
5 ) Gardner's syndrome
ANSWER 2
Wednesday, July 19, 2006
CT brain in MRCP
There are a few important and popular CTs brain that are commonly asked in MRCP exams esepcially in Part 2,there are a few basic principles to remember,
1) Acute haemorrhage appears to be hyperdense (white) in CT brain,
2) Chronic haemorrhage appears to be hypodense (black),
Condition 1: Cerebral toxoplasmosis
1) Acute haemorrhage appears to be hyperdense (white) in CT brain,
2) Chronic haemorrhage appears to be hypodense (black),
Condition 1: Cerebral toxoplasmosis

A few clues to the diagnosis,
1) Young patients with unexplained headache, fever,seizure,neurological deficit and increased intracranial pressure.
2) CTbrain shows ring enhancing lesion after IV contrast ( 30% unilocular but majority multilocular)
3) 75% at basal ganglia, occurs when CD4 less than 100.
Condition 2: Subdural Haematoma

Above image shows acute subdural haematoma ( white)
 Above image shows chronic subdural haematoma (black)
Above image shows chronic subdural haematoma (black)
Usually in alcoholic and elderly patients. If it is acute, it appears to be hyperdense or lese it is hypodense in chronic lesion
Condition 3: Extradural Haematoma

Usually after motor vehicle accident or trauma. Remember about possibility of lucid interval.
Condititon 4: Stroke ( Ischaemic or Haemorrahgic stroke)
Simple to pick up in CT brain if it is massive, however, remember that CT scan may not have obvious changes in ischaemic stroke patients if less than 6 hours. ( Time required for the brain parenchyma to liquidfy after infarct to be shown in CT)
More photo based questions are coming...........
Sunday, July 16, 2006
More MRCP Part 2 questions
QUESTIONS ABOUT NEPHROLOGY
1) A cachectic 77-year-old man is admitted with NAUSEA NAD VOMITTING and is found to have blood investigations as below,
creatinine =520 micro mol/l
BU=15mmol/l
Na=145 mmol/l
K=5.2 mmol/l
He has been on a number of medications. Which of the following drugs need adjustment or should be avioded EXCEPT
A : Ibuprofen
B : Peridonpril
C : Allopurinol
D : Lansoprazole
E : Metformin
ANSWER: D
2)A 38-year-old woman with a renal transplant is established on cyclosporin, azathioprine and prednisolone to prevent transplant rejection, and enalapril and bendrofluazide for hypertension. After a 14-day course of ketoconazole for oesophageal candidiasis her creatinine is found to have increased from 100 mmol/L to 400 mmol/L.
Her deterioration in renal function is most likely attributable to:
A : hypertension poorly controlled on enalapril and bendrofluazide
B : nephrotoxic effects of ketoconazole
C : ciclosporin toxicity due to inhibition of ciclosporin metabolism by ketoconazole
D : transplant rejection due to induction of ciclosporin metabolism by ketoconazole
E : effect of enalapril on background of stenosis of artery supplying renal transplant.
ANSWER:C
3) A 22-year-old woman consults her general practitioner in the 10th week of her pregnancy.
She complains of fever and dysuria. There is no other significant history but direct questioning reveals a self-limiting rash in the past after taking penicillin. Her GP sends off a sample of urine that shows a significant growth of Gram negative bacilli. The organism is sensitive to the antibiotics listed below.
What is your next plan of action?
A : Give Ciprofloxacin
B : Avoid treatment since she may allergic to other antibiotics as well.
C : Cefaclor
D : Trimethoprim
E : Gentamicin
ANSWER: C
4)In type IV renal tubal acidosis
A there is normal renal handling of K+ and H+
B it is helped by fludrocortisone
C it is associated with an increased GFR
D it is associated with aminoaciduria
E there is increased bicarbonate in the urine
ANSWER: B
5)Which of the following is true concerning a 68 year old male with type 2 diabetes diagnosed with type IV renal tubal acidosis?
1 ) Aminoaciduria would be expected.
2 ) Fludrocortisone treatment is effective
3 ) Increased Glomerular filtration rate is expected.
4 ) Increased urinary bicarbonate would be expected.
5 ) Normal renal handling of K+ and H+
ANSWER: B
6)Recognised features of renal tubular acidosis include except:
A an inability to excrete hydrogen ions in type I renal tubular acidosis
B only occurs in patients with diabetes if Type IV
C a urine pH of less than six
D nephrocalcinosis
E hyperchloraemia
ANSWER: B
7)Features of distal type IV renal tubular acidosis include:
A Increased anion gap and aminoaciduria.
B Hyperchloraemic acidosis with hypokalaemia.
C Decreased GFR
D Normal renal excretion of hydrogen and potassium ions.
E Plasma bicarbonate concentrations usually less than 15 mmol/L (20-26).
ANSWER: C
8)The following symptoms occur in a patient with renal tubular acidosis EXCEPT:
A muscle cramps
B loin pain on micturition
C constipation
D dizzeness on standing up suddenly
E nausea and vomitting
ANSWER: E
9) Type 1 renal tubular acidoses is associated with EXCEPT:
A a urinary pH of less than 5.3 in the presence of systemic acidaemia
B nephrocalcinosis
C growth retardation
D Sjogren's syndrome
E chronic obstructive uropathy
ANSWER: A
MORE MRCP QUESTIONS ARE COMING.......
1) A cachectic 77-year-old man is admitted with NAUSEA NAD VOMITTING and is found to have blood investigations as below,
creatinine =520 micro mol/l
BU=15mmol/l
Na=145 mmol/l
K=5.2 mmol/l
He has been on a number of medications. Which of the following drugs need adjustment or should be avioded EXCEPT
A : Ibuprofen
B : Peridonpril
C : Allopurinol
D : Lansoprazole
E : Metformin
ANSWER: D
2)A 38-year-old woman with a renal transplant is established on cyclosporin, azathioprine and prednisolone to prevent transplant rejection, and enalapril and bendrofluazide for hypertension. After a 14-day course of ketoconazole for oesophageal candidiasis her creatinine is found to have increased from 100 mmol/L to 400 mmol/L.
Her deterioration in renal function is most likely attributable to:
A : hypertension poorly controlled on enalapril and bendrofluazide
B : nephrotoxic effects of ketoconazole
C : ciclosporin toxicity due to inhibition of ciclosporin metabolism by ketoconazole
D : transplant rejection due to induction of ciclosporin metabolism by ketoconazole
E : effect of enalapril on background of stenosis of artery supplying renal transplant.
ANSWER:C
3) A 22-year-old woman consults her general practitioner in the 10th week of her pregnancy.
She complains of fever and dysuria. There is no other significant history but direct questioning reveals a self-limiting rash in the past after taking penicillin. Her GP sends off a sample of urine that shows a significant growth of Gram negative bacilli. The organism is sensitive to the antibiotics listed below.
What is your next plan of action?
A : Give Ciprofloxacin
B : Avoid treatment since she may allergic to other antibiotics as well.
C : Cefaclor
D : Trimethoprim
E : Gentamicin
ANSWER: C
4)In type IV renal tubal acidosis
A there is normal renal handling of K+ and H+
B it is helped by fludrocortisone
C it is associated with an increased GFR
D it is associated with aminoaciduria
E there is increased bicarbonate in the urine
ANSWER: B
5)Which of the following is true concerning a 68 year old male with type 2 diabetes diagnosed with type IV renal tubal acidosis?
1 ) Aminoaciduria would be expected.
2 ) Fludrocortisone treatment is effective
3 ) Increased Glomerular filtration rate is expected.
4 ) Increased urinary bicarbonate would be expected.
5 ) Normal renal handling of K+ and H+
ANSWER: B
6)Recognised features of renal tubular acidosis include except:
A an inability to excrete hydrogen ions in type I renal tubular acidosis
B only occurs in patients with diabetes if Type IV
C a urine pH of less than six
D nephrocalcinosis
E hyperchloraemia
ANSWER: B
7)Features of distal type IV renal tubular acidosis include:
A Increased anion gap and aminoaciduria.
B Hyperchloraemic acidosis with hypokalaemia.
C Decreased GFR
D Normal renal excretion of hydrogen and potassium ions.
E Plasma bicarbonate concentrations usually less than 15 mmol/L (20-26).
ANSWER: C
8)The following symptoms occur in a patient with renal tubular acidosis EXCEPT:
A muscle cramps
B loin pain on micturition
C constipation
D dizzeness on standing up suddenly
E nausea and vomitting
ANSWER: E
9) Type 1 renal tubular acidoses is associated with EXCEPT:
A a urinary pH of less than 5.3 in the presence of systemic acidaemia
B nephrocalcinosis
C growth retardation
D Sjogren's syndrome
E chronic obstructive uropathy
ANSWER: A
MORE MRCP QUESTIONS ARE COMING.......
Breakdown of MRCP Part 1Qs
Breakdown of MRCP Part 1 questions according to specialty in 2003 (Diet 3),
Total questions: 199
1) Cardiology 15
2) Clinical haematology and oncology 15
3) Pharmacology and therapeutics 20
4) Clinical science 25
5) Dermatology 8
6) Endocrinology 15
7) Gastroenterology 15
8) Infectious disease and STD 14
9) Nephrology 15
10) Neurology 15
11) Ophthalmology 4
12) Psychitry 8
13) Respiratory medicine 15
14) Rheumatology 15
so.... what is the difference between Part 1 and 2? I think a few important points candidates must take note...
1) More questions about basic science are asked in Part 1 than Part 2. These questions include basic pharmacology such as side effects, pharmacokinetics and pharmacodynamics.
2) More questions about management of certain diseases are asked in Part 2. Therefore candidates should use more time to learn about the management in Part 2.
3) It is more difficult to pass Part 1 than Part 2. The passing rate in Part 1 is around 30% compared to Part 2 ( about 50%). This due to candidates' poor performance in answering basic science/pharmacology questions!
Total questions: 199
1) Cardiology 15
2) Clinical haematology and oncology 15
3) Pharmacology and therapeutics 20
4) Clinical science 25
5) Dermatology 8
6) Endocrinology 15
7) Gastroenterology 15
8) Infectious disease and STD 14
9) Nephrology 15
10) Neurology 15
11) Ophthalmology 4
12) Psychitry 8
13) Respiratory medicine 15
14) Rheumatology 15
so.... what is the difference between Part 1 and 2? I think a few important points candidates must take note...
1) More questions about basic science are asked in Part 1 than Part 2. These questions include basic pharmacology such as side effects, pharmacokinetics and pharmacodynamics.
2) More questions about management of certain diseases are asked in Part 2. Therefore candidates should use more time to learn about the management in Part 2.
3) It is more difficult to pass Part 1 than Part 2. The passing rate in Part 1 is around 30% compared to Part 2 ( about 50%). This due to candidates' poor performance in answering basic science/pharmacology questions!
Tuesday, July 11, 2006
Articles About MRCP
Monday, July 10, 2006
Popular Drugs in MRCP (4)
As in my previous posts, I have discussed 3 most popular drugs in MRCP ie warfarin, digoxin and amiodarone. Today I would talk about antithyroid drugs. There are 2 main antithyroid drugs available namely propylthiouracil (PTU) and methimazole, or carbimazole, a derivative of methimazole which is commonly used in UK and Europe.
Commonly asked questions in MRCP are about the side effects of these drugs, remember that both drugs have quite similar side effects, these side effects are,
a) Rashes
b) Hepatitis and cholestatic jaundice
c) Agranulocytosis ( patients usually present with severe sorethroat!)
Remember and learn how to intepret T4/TSH results after treatment. This is commonly asked in exam as well!
Commonly asked questions in MRCP are about the side effects of these drugs, remember that both drugs have quite similar side effects, these side effects are,
a) Rashes
b) Hepatitis and cholestatic jaundice
c) Agranulocytosis ( patients usually present with severe sorethroat!)
Remember and learn how to intepret T4/TSH results after treatment. This is commonly asked in exam as well!
Books for MRCP Part 2
There are a few important books for MRCP Part 2. Get these books before your part 2,
1) Handbook for the MRCP Part 2 Examination by Sanjay Sharma
2) 100 Diseases for the MRCP Part 2 by Miles Witham
3) A Guide to the MRCP, Part 2 Written Paper by Anthony Warrens
4) Essential Revision Notes For MRCP by Kalra
Good Luck for your Exam!
1) Handbook for the MRCP Part 2 Examination by Sanjay Sharma
2) 100 Diseases for the MRCP Part 2 by Miles Witham
3) A Guide to the MRCP, Part 2 Written Paper by Anthony Warrens
4) Essential Revision Notes For MRCP by Kalra
Good Luck for your Exam!
Sunday, July 09, 2006
Renal Tubular Acidosis in MRCP (2)
From previous post……
RENAL TUBULAR ACIDOSIS TYPE II
RTA type II is also known as proximal RTA, it is due to failure of proximal tubule to re-absorb HCO3. It is less common than RTA type I . It is most commonly occurs as part of generalized proximal tubular defect that results in glycosuria, aminoaciduria, phosphaturia and renal tubular acidoisis- the Fanconi syndrome.
Causes of proximal RTA can be due to congenital or acquired causes.
Congenital causes are Hereditary, Wilson’s disease, Cystinosis and fructose intolerance.
Acquired causes are autoimmune disease ( such as Sjogren’s), drugs ( lead, tetracycline), myeloma, amyloid, hyperparathyroidism and nephrotic syndrome.
PROXIMAL- hyperParathyroidism, Renal ( nephrotic syndrome, interstitial nephritis), OX ( others- drugs- tetracycline), I ( autoimmune) ,Myeloma, Amyloid and Lead!
A few important points to remember,
1)calculus formation is uncommon in proximal RTA and
2)plasma HCO3 tens to be higher!
RTA type III
Combination of type I and II- very rare, seldom asked in MRCP
RENAL TUBULAR ACIDOSIS TYPE IV
The commonest type of RTA. Patients are acidotic and HYPERKALEMIA!
It is known as hyporeninaemic hypoaldosteronism. It is common associated with diabetic nephropathy. The defect is caused either by hypoaldosteronism or renal resistance to the effect of aldosterone!
RENAL TUBULAR ACIDOSIS TYPE II
RTA type II is also known as proximal RTA, it is due to failure of proximal tubule to re-absorb HCO3. It is less common than RTA type I . It is most commonly occurs as part of generalized proximal tubular defect that results in glycosuria, aminoaciduria, phosphaturia and renal tubular acidoisis- the Fanconi syndrome.
Causes of proximal RTA can be due to congenital or acquired causes.
Congenital causes are Hereditary, Wilson’s disease, Cystinosis and fructose intolerance.
Acquired causes are autoimmune disease ( such as Sjogren’s), drugs ( lead, tetracycline), myeloma, amyloid, hyperparathyroidism and nephrotic syndrome.
PROXIMAL- hyperParathyroidism, Renal ( nephrotic syndrome, interstitial nephritis), OX ( others- drugs- tetracycline), I ( autoimmune) ,Myeloma, Amyloid and Lead!
A few important points to remember,
1)calculus formation is uncommon in proximal RTA and
2)plasma HCO3 tens to be higher!
RTA type III
Combination of type I and II- very rare, seldom asked in MRCP
RENAL TUBULAR ACIDOSIS TYPE IV
The commonest type of RTA. Patients are acidotic and HYPERKALEMIA!
It is known as hyporeninaemic hypoaldosteronism. It is common associated with diabetic nephropathy. The defect is caused either by hypoaldosteronism or renal resistance to the effect of aldosterone!
Friday, July 07, 2006
Renal Tubular Acidosis in MRCP (1)
As I mentioned earlier in my previous post, there are two main types of metabolic acidosis. These can be either a normal or reduced anion gap type of metabolic acidosis. The causes of reduced anion gap metabolic acidosis are MUD-PILES. Today we are going to discuss the major cause of normal anion gap metabolic acidosis namely RENAL TUBULAR ACIDOSIS. In case you forget,
Anion gap= (Na+K) - (Cl+HCO3)
Normal range= 10-18 mmol/L
In above formula, as you notice, in metabolic acidosis, the value of HCO3 will be reduced, therefore, in a normal anion gap metabolic acidosis, the value of Cl will be increased so that the value of anion gap remains unchanged, therefore, normal anion gap metabolic acidosis also can be named as hyperchloraemic acidosis.
RENAL TUBULAR ACIDOSIS TYPE 1
It is the commonest RTA. It is known as distal RTA. It is due to failure of the kidney to create acid urine because the distal tubule fails to exchange Na for H.
Remember that RTA can be due to either congenital or acquired. For RTA type I causes for acquired one include DISTAL+O
D - Vit D excess
I -Inflammatory/ autoimmune- such as chronic active hepatitis, Sjogren’s syndrome.
S -Sickle Cell Disease
T -Transplanted kidney
A -Amphotericin, analgesics (drugs)
L -Lithium
O -Others- medullary sponge kidney
Remember a few features that are characteristics to distal RTA, they are,
1)Hypercalciuria and risk of stone formation and nephrocalcinosis,
2)Plasma HCO3 tends to be lower than proximal,
3)Urine PH always more than 5.5
to be continued......................
Anion gap= (Na+K) - (Cl+HCO3)
Normal range= 10-18 mmol/L
In above formula, as you notice, in metabolic acidosis, the value of HCO3 will be reduced, therefore, in a normal anion gap metabolic acidosis, the value of Cl will be increased so that the value of anion gap remains unchanged, therefore, normal anion gap metabolic acidosis also can be named as hyperchloraemic acidosis.
RENAL TUBULAR ACIDOSIS TYPE 1
It is the commonest RTA. It is known as distal RTA. It is due to failure of the kidney to create acid urine because the distal tubule fails to exchange Na for H.
Remember that RTA can be due to either congenital or acquired. For RTA type I causes for acquired one include DISTAL+O
D - Vit D excess
I -Inflammatory/ autoimmune- such as chronic active hepatitis, Sjogren’s syndrome.
S -Sickle Cell Disease
T -Transplanted kidney
A -Amphotericin, analgesics (drugs)
L -Lithium
O -Others- medullary sponge kidney
Remember a few features that are characteristics to distal RTA, they are,
1)Hypercalciuria and risk of stone formation and nephrocalcinosis,
2)Plasma HCO3 tends to be lower than proximal,
3)Urine PH always more than 5.5
to be continued......................
Tuesday, July 04, 2006
Tuberculosis in MRCP
Tuberculosis is one of the popular MRCP questions. It is caused by Mycobacterium tubeculosis and in 1993, WHO declared TB as a global emergency. It was discovered by Robert Koch in 1905.to learn more about Robert Koch, click here !
Common questions asked in MRCP are about the treatment of tuberculosis and its side effects, first line medications for TB and their side effects are as follow,
a) Isoniazid- peripheral neuropathy, hepatitis, pyridoxine deficiency, agranulocytosis, drug-induced lupus!
b) Rifampicin-cholestatic jaundice, orange urine, thrombocytopenia, enzyme inducer ( make OCP less effective).
c) Ethambutol-optic neuritis ( yellow/green colour defect)
d)Pyrazinamide-hepatitis, hyperuricaemia ( causes gout)
e) Streptomycin-ototoxicity and nephrotoxicity.
Duration of treatment usually 6 months for pulmonary TB and more than 6 months for extra-pulmonary. ( Regime usually consists of 2 months intensive daily treatment and 4 months or more for biweekly maintenance treatment)
Questions about co-infection of HIV and TB are becoming more and more popular and challenging in MRCP. I would talk abou this in future posts!
Common questions asked in MRCP are about the treatment of tuberculosis and its side effects, first line medications for TB and their side effects are as follow,
a) Isoniazid- peripheral neuropathy, hepatitis, pyridoxine deficiency, agranulocytosis, drug-induced lupus!
b) Rifampicin-cholestatic jaundice, orange urine, thrombocytopenia, enzyme inducer ( make OCP less effective).
c) Ethambutol-optic neuritis ( yellow/green colour defect)
d)Pyrazinamide-hepatitis, hyperuricaemia ( causes gout)
e) Streptomycin-ototoxicity and nephrotoxicity.
Duration of treatment usually 6 months for pulmonary TB and more than 6 months for extra-pulmonary. ( Regime usually consists of 2 months intensive daily treatment and 4 months or more for biweekly maintenance treatment)
Questions about co-infection of HIV and TB are becoming more and more popular and challenging in MRCP. I would talk abou this in future posts!
Infections in MRCP Part 2
Questions about common infections in MRCP......
1)A 20-year-old man undergoes successful renal transplantation with a matched related donor graft. One month later he presents with a high fever and leukopoenia. He becomes dyspnoeic. Liver function tests are markedly deranged.
Which of the following is the most likely cause of his illness?
1 ) Adenovirus 2 ) Coxsackievirus 3 ) Cytomegalovirus
4 ) Influenza virus 5 ) Parvovirus B19
ANSWER: 3
2) A 22-year-old girl with sickle cell disease presents with pain in her left thigh. A plain X-ray film shows changes consistent with osteomyelitis of the left femur.
Which of the following is the most likely causative organism?
1 ) Clostridium perfringens 2 ) Enterococcus faecium 3 ) Listeria monocytogenes 4 ) Staphylococcus aureus 5 ) Salmonella enteritiditis
ANSWER: 5
3)A 23-year-old man is noted by his partner to be jaundiced. Two weeks previously he suffered a mild flu-like illness. His investigations are shown.Hb 7.3 g/dlMCV 99 fLWCC 8.0x109/LPlt 340x109/LReticulocytes 6.8%Albumin 41 g/LTotal Bilirubin 42 µmol/LAST 36 IU/LALP 40 IU/LUrine dipstick urobilinogen ++, bilurubin negative, protein negative, blood ++
What antiobiotics would be useful in treating his condition?
1 ) ampicillin 2 ) macrolides 3 ) aminoglycosides 4 ) cephalosporins 5 ) penicillin
ANSWER: 2
4)A 23-year-old Indian man is diagnosed with pulmonary tuberculosis and is started on rifampicin, isoniazid, and pyrazinamide. Four weeks later he presents with fever, myalgia, and lethargy.Investigations:Haemoglobin 14.5 g/dLWBC 7.5 x 109/LNeutrophils 5.5 x 109/LLymphocytes 0.8 x 109/LMonocytes 0.05 x 109/LEosinophils 1.14 x 109/LBasophils 0.01 x 109/LPlatelets 350 x 109/LSerum sodium 141 mmol/LSerum potassium 5.1 mmol/L Serum urea 27.9 mmol/LSerum creatinine 400 umol/LSerum bilirubin 7umol/L Serum aspartate transaminase 31 IU/LSerum alkaline phosphatase 97 IU/LSerum albumin 39 g/LUrinalysis Protein +, Leucocytes +, no bacteriaUrine culture Negative
What is the most likely cause of his renal impairment?
1 ) Acute interstitial nephritis 2 ) Isoniazid toxicity 3 ) Plasmodium vivax malaria 4 ) Renal tuberculosis 5 ) Rhabdomyolysis
ANSWER: 1
5)A 27 year old man presents with complaints of pains in multiple joints one weeks after returning from a holiday in Thailand. He describes flitting arthralgia beginning I both knees, migrating to both wrists intermittently. His main complaint is of more severe pain in his left knee. On examination, he is febrile 38.5°C. The left knee is swollen, warm and tender. Several pustular lesions are noted on three digits of his right hand.InvestigationsHb 14.8 g/dlWCC 12.3 x 109/lPlatelets 450 x 109/lPlasma sodium 141 mmol/lPlasma potassium 4.9 mmol/lPlasma urea 3.8 mmol/lPlasma creatinine 116 mmol/lAntinuclear antibody NegativeRheumatoid factor NegativeBlood cultures NegativeKnee aspiration: Microscopy Yellow turbid fluid. Numerous polymorphs.Culture Negative Gram stain of the synovial fluid is likely to show:
1 ) Gram negative bacilli 2 ) Gram negative coccobacillus 3 ) Gram negative intracellular diplococci 4 ) Gram positive cocci in clusters 5 ) Negatively birefringent crystals
ANSWER: 3
6)A 26-year-old homosexual man presented to hospital with a fever, dry cough and dyspnoea. Oropharyngeal candidiasis was noted. He was found to be HIV antibody positive and Pneumocystis carinii was found on bronchoalveolar lavage. His Pneumocystis carinii pneumonia (PCP) was treated with intravenous co-trimoxazole and he was subsequently started on highly active antiretroviral therapy (HAART).Four weeks later he presented to clinic complaining of weakness and generalised aching. He was taking highly active antiretroviral therapy (zidovudine (AZT), lamivudine (3TC), nelfinavir), co-trimoxazole as Pneumocystis carinii prophylaxis and fluconazole.Investigations:Serum creatine kinase 900 IU/l (24-195)
What is the cause of this problem?
1 ) Co-trimoxazole 2 ) Fluconazole 3 ) Lamivudine (3TC) 4 ) Nelfinavir 5 ) Zidovudine (AZT)
ANSWER:5
1)A 20-year-old man undergoes successful renal transplantation with a matched related donor graft. One month later he presents with a high fever and leukopoenia. He becomes dyspnoeic. Liver function tests are markedly deranged.
Which of the following is the most likely cause of his illness?
1 ) Adenovirus 2 ) Coxsackievirus 3 ) Cytomegalovirus
4 ) Influenza virus 5 ) Parvovirus B19
ANSWER: 3
2) A 22-year-old girl with sickle cell disease presents with pain in her left thigh. A plain X-ray film shows changes consistent with osteomyelitis of the left femur.
Which of the following is the most likely causative organism?
1 ) Clostridium perfringens 2 ) Enterococcus faecium 3 ) Listeria monocytogenes 4 ) Staphylococcus aureus 5 ) Salmonella enteritiditis
ANSWER: 5
3)A 23-year-old man is noted by his partner to be jaundiced. Two weeks previously he suffered a mild flu-like illness. His investigations are shown.Hb 7.3 g/dlMCV 99 fLWCC 8.0x109/LPlt 340x109/LReticulocytes 6.8%Albumin 41 g/LTotal Bilirubin 42 µmol/LAST 36 IU/LALP 40 IU/LUrine dipstick urobilinogen ++, bilurubin negative, protein negative, blood ++
What antiobiotics would be useful in treating his condition?
1 ) ampicillin 2 ) macrolides 3 ) aminoglycosides 4 ) cephalosporins 5 ) penicillin
ANSWER: 2
4)A 23-year-old Indian man is diagnosed with pulmonary tuberculosis and is started on rifampicin, isoniazid, and pyrazinamide. Four weeks later he presents with fever, myalgia, and lethargy.Investigations:Haemoglobin 14.5 g/dLWBC 7.5 x 109/LNeutrophils 5.5 x 109/LLymphocytes 0.8 x 109/LMonocytes 0.05 x 109/LEosinophils 1.14 x 109/LBasophils 0.01 x 109/LPlatelets 350 x 109/LSerum sodium 141 mmol/LSerum potassium 5.1 mmol/L Serum urea 27.9 mmol/LSerum creatinine 400 umol/LSerum bilirubin 7umol/L Serum aspartate transaminase 31 IU/LSerum alkaline phosphatase 97 IU/LSerum albumin 39 g/LUrinalysis Protein +, Leucocytes +, no bacteriaUrine culture Negative
What is the most likely cause of his renal impairment?
1 ) Acute interstitial nephritis 2 ) Isoniazid toxicity 3 ) Plasmodium vivax malaria 4 ) Renal tuberculosis 5 ) Rhabdomyolysis
ANSWER: 1
5)A 27 year old man presents with complaints of pains in multiple joints one weeks after returning from a holiday in Thailand. He describes flitting arthralgia beginning I both knees, migrating to both wrists intermittently. His main complaint is of more severe pain in his left knee. On examination, he is febrile 38.5°C. The left knee is swollen, warm and tender. Several pustular lesions are noted on three digits of his right hand.InvestigationsHb 14.8 g/dlWCC 12.3 x 109/lPlatelets 450 x 109/lPlasma sodium 141 mmol/lPlasma potassium 4.9 mmol/lPlasma urea 3.8 mmol/lPlasma creatinine 116 mmol/lAntinuclear antibody NegativeRheumatoid factor NegativeBlood cultures NegativeKnee aspiration: Microscopy Yellow turbid fluid. Numerous polymorphs.Culture Negative Gram stain of the synovial fluid is likely to show:
1 ) Gram negative bacilli 2 ) Gram negative coccobacillus 3 ) Gram negative intracellular diplococci 4 ) Gram positive cocci in clusters 5 ) Negatively birefringent crystals
ANSWER: 3
6)A 26-year-old homosexual man presented to hospital with a fever, dry cough and dyspnoea. Oropharyngeal candidiasis was noted. He was found to be HIV antibody positive and Pneumocystis carinii was found on bronchoalveolar lavage. His Pneumocystis carinii pneumonia (PCP) was treated with intravenous co-trimoxazole and he was subsequently started on highly active antiretroviral therapy (HAART).Four weeks later he presented to clinic complaining of weakness and generalised aching. He was taking highly active antiretroviral therapy (zidovudine (AZT), lamivudine (3TC), nelfinavir), co-trimoxazole as Pneumocystis carinii prophylaxis and fluconazole.Investigations:Serum creatine kinase 900 IU/l (24-195)
What is the cause of this problem?
1 ) Co-trimoxazole 2 ) Fluconazole 3 ) Lamivudine (3TC) 4 ) Nelfinavir 5 ) Zidovudine (AZT)
ANSWER:5
Sunday, July 02, 2006
MRCP Part 1 Questions
Hope you find these questions useful........... For MRCP Part 1
1)Which of the following is true regarding diabetic neuropathy?
A : It is best detected by testing for light touch with cotton wool.
B : It is always bilateral.
C : It does not cause vomiting.
D : It does not cause urinary incontinence.
E : It cannot be reversed by good glycaemic control.
ANSWER: E
2) A 76-year-old man presents with an acute confusional state. He was diagnosed to have lung cancer recently.Investigations review serum calcium 3.21 mmol/l. Which is the most appropriate initial treatment?
A : Intravenous sodium pamidronate
B : Intravenous 5% dextrose
C : Oral prednisolone (20-60 mg)
D : Intravenous frusemide
E : Intravenous 0.9% sodium chloride.
ANSWER: E
3)The presence of ketoacidosis in a patient without diabetes mellitus would suggest which one of the following causes?
A : Insulinoma
B : Addisonian crisis
C : Starvation
D : Acute on chronic renal failure
E : Salicylate overdose.
ANSWER: C
To learn more about metabolic acidosis, look at my previous post of Metabolic Acidosis in MRCP!
4)A 60-year-old man presents with breathlessness. He has had a history of previous myocardial infarction and peripheral vascular disease. He has recently been started on PERINDOPRIL for hypertension. He has been anuric for 2 hour. His serum urea is 35 mmol/l and his potassium is 7 .9 mmol/l. His ECG shows tall tented T waves. The first most appropriate step in management would be:
A : ten units of soluble insulin with 50g glucose(50%) IV
B : haemodialysis
C : bicarbonate (50 mls of a 4.2% solution) by IVI
D : calcium resonium 30g
E : 10-30 ml calcium gluconate (10%) IVI.
ANSWER: E
5) Which one of these features is typical of dermatomyositis...EXCEPT?
A : Heliotrope rash around the eye
B : Gottron's papules over knuckles of fingers
C : proximal muscle weakness
D : association with malignancy
E : Sclerotic digital skin.
ANSWER: E
6)
1)Which of the following is true regarding diabetic neuropathy?
A : It is best detected by testing for light touch with cotton wool.
B : It is always bilateral.
C : It does not cause vomiting.
D : It does not cause urinary incontinence.
E : It cannot be reversed by good glycaemic control.
ANSWER: E
2) A 76-year-old man presents with an acute confusional state. He was diagnosed to have lung cancer recently.Investigations review serum calcium 3.21 mmol/l. Which is the most appropriate initial treatment?
A : Intravenous sodium pamidronate
B : Intravenous 5% dextrose
C : Oral prednisolone (20-60 mg)
D : Intravenous frusemide
E : Intravenous 0.9% sodium chloride.
ANSWER: E
3)The presence of ketoacidosis in a patient without diabetes mellitus would suggest which one of the following causes?
A : Insulinoma
B : Addisonian crisis
C : Starvation
D : Acute on chronic renal failure
E : Salicylate overdose.
ANSWER: C
To learn more about metabolic acidosis, look at my previous post of Metabolic Acidosis in MRCP!
4)A 60-year-old man presents with breathlessness. He has had a history of previous myocardial infarction and peripheral vascular disease. He has recently been started on PERINDOPRIL for hypertension. He has been anuric for 2 hour. His serum urea is 35 mmol/l and his potassium is 7 .9 mmol/l. His ECG shows tall tented T waves. The first most appropriate step in management would be:
A : ten units of soluble insulin with 50g glucose(50%) IV
B : haemodialysis
C : bicarbonate (50 mls of a 4.2% solution) by IVI
D : calcium resonium 30g
E : 10-30 ml calcium gluconate (10%) IVI.
ANSWER: E
5) Which one of these features is typical of dermatomyositis...EXCEPT?
A : Heliotrope rash around the eye
B : Gottron's papules over knuckles of fingers
C : proximal muscle weakness
D : association with malignancy
E : Sclerotic digital skin.
ANSWER: E
6)

Photo source: www.passpaces.com/MRCP/issue2.html
The 25-year-old lady is admitted with ptosis, diplopia and dysphagia. On examination he is found to have fatigable muscle weakness and
normal deep tendon reflexes. What is the most likely diagnosis?
A : Bell’s palsy
B : Guillain-Barre syndrome
C : Motor neurone disease
D : Multiple sclerosis
E : Myasthenia gravis.
ANSWER: E
Saturday, July 01, 2006
Dermatology in MRCP (3)
Other important skin problems in MRCP......
7) Pemphigus/pemphigoid
7) Pemphigus/pemphigoid
 Two common autoimmune bullous diseases. Remember that pemphigus is described as flaccid, thin roofed blisters involving the mucosal membrane and the blisters have tendency to rupture. (Pemphigus also has positive Nikolsky's sign). For pemphigoid, it is described as multiple tense blisters. (such as in above photo)
Two common autoimmune bullous diseases. Remember that pemphigus is described as flaccid, thin roofed blisters involving the mucosal membrane and the blisters have tendency to rupture. (Pemphigus also has positive Nikolsky's sign). For pemphigoid, it is described as multiple tense blisters. (such as in above photo)
8) Porphyria cutanea tarda
 The blisters and vesicles usually occur on sun-exposed areas. Classically described over the hand. To learn more about porphyria, click here !
The blisters and vesicles usually occur on sun-exposed areas. Classically described over the hand. To learn more about porphyria, click here !
9) Psoriasis
 Clasically described as 'well dermacated salmon pink plaque with silvery white scales'. There are a few subtypes of psoriasis, to learn more, click here!
Clasically described as 'well dermacated salmon pink plaque with silvery white scales'. There are a few subtypes of psoriasis, to learn more, click here!
Subscribe to:
Posts (Atom)
