
This patient presented to us with fever and painful swallowing, what can you see in his oral cavity?
Yes, you are right, oral candidiasis is common among HIV patients. However, you must remember that it is not a AIDS defining disease because you can find this problem in other immunosuppresed patients such as in diabetic patients and patients after chemotheraphy. Anyway, oesophageal candidiasis is an AIDS defining disease in which I think this patient may be having in view of history of painful swallowing.
Common questions in MRCP part 1 and 2 are types of diseases HIV patients will get according to their CD4 counts. One of the most popular question is PCP. Always remember that HIV patients will get PCP once their CD4 is lee than 200! Other common questions are as follow,
1)A 24-year-old man presented with a ten-week history of progressively worsening exertional dyspnoea and a dry cough. Auscultation of his chest revealed fine inspiratory crackles to the mid-zones. He was afebrile. His chest radiograph is shown below. A Heaf test was negative. 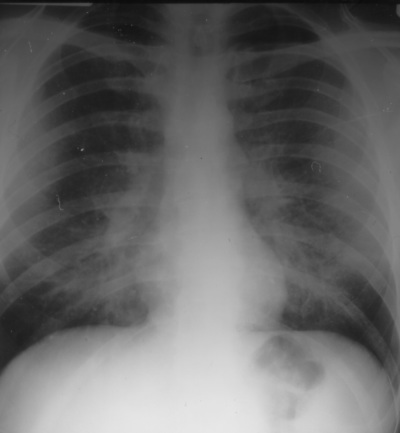
Which of the following investigations will be most helpful in establishing a diagnosis?
1 ) Abdominal ultrasound scan 2 ) Atypical serology
3 ) Bone marrow aspiration 4 ) Bronchoalveolar lavage
5 ) CD4 T-lymphocyte count 6 ) Cytoplasmic antineutrophil cytoplasmic antibody (cANCA)
7 ) C-reactive protein (CRP) 8 ) Erythrocyte sedimentation rate (ESR)
9 ) HIV antibody test 10 ) Peak flow rate
11 ) Plasma lactate dehydrogenase (LDH) 12 ) Sputum culture
13 ) Transbronchial lung biopsy 14 ) Trial of steroids
15 ) 24 hour urinary calcium excretion
ANSWER: 9,13, 15 (POSSIBILITY OF SARCOIDOSIS! CXR CAN BE SIMILIAR TO PCP)
2)This HIV positive man presented with cough, haemoptysis and a rash (shown).
What is the causative agent? 
1 ) Mycobacterium tuberculosis 2 ) Pneumocystis carinii
3 ) Cytomegalovirus 4 ) Epstein-Barr virus
5 ) Human herpesvirus-8
ANSWER: 5
3) A 35 year-old man is admitted with a three week history of progressively worsening dyspneoa accompanied by a non-productive cough. For the 24 hours prior to admission he has been dyspnoeic at rest. He also reports having occasional 'chills' and has felt febrile on occasions.He has no other past medical history of note. He works as an accountant with the local authority. He smokes 20 cigarettes per day and occasionally smokes cannabis. He drinks 18-20 units of alcohol per week. He is divorced and currently lives alone.He says that his diet has been poor since he separated from his wife 2 years previously; in this time he has lost about 2 stones in weight. He does not take any regular medication.On examination he is dyspnoeic at rest with a respiratory rate of 22/minute. He is febrile, 38°C. His chest is clear on auscultation.
Which of the following test results would most strongly support a diagnosis of Pneumocystis carinii pneumonia?
1 ) Low absolute lymphocyte count 2 ) Lobar consolidation on the chest radiograph 3 ) Oxygen desaturation on exercise 4 ) A normal chest X-ray 5 ) Past history of homosexual contact
ANSWER: 3
4)A 44-year-old HIV seropositive patient is seen in a routine outpatient appointment. He was diagnosed with HIV disease two years ago when he presented with Pneumocystis carinii pneumonia (PCP) with a CD4 T-lymphocyte count of 40 cells/mm3. After being treated for PCP he was started on combination antiretroviral therapy. His initial response to antiretroviral therapy had been promising, with an increase in his CD4 count (210 cells/mm3) and achieving an undetectable HIV viral load in the peripheral blood. One year ago, his CD4 count started to fall and HIV RNA became detectable in peripheral blood. An HIV viral resistance test confirmed resistance to all of his antiretroviral drugs. The patient admitted that over the preceeding three months that he had only been taking his therapy intermittently. Despite the risks, he decided that he did not wish to have any further antiviral therapy. At this point, his CD4 count was 20 cells/mm3 with a very high HIV viral load of 120,000 copies/ml.Seven months ago he presented with malaise, weight loss (8kg), fevers and night sweats. Mycobacterium avium intracellulare (MAI) was isolated from a blood culture and he was started on therapy with ethambutol and rifabutin. He subsequently agreed to re-start antiretroviral therapy.During his clinic consultation, he states that he has noticed a steady deterioration in his visual acuity over the past four weeks. His current medications include stavudine (d4T), didanosine (ddI), nevirapine, ethambutol, and rifabutin. On examination, fundoscopy is normal.His last CD4 count, taken one month ago was 30 cells/mm3, with an HIV viral load of 2500 copies/ml.
What is the most likely cause of his reduction in visual acuity?
1 ) Antiretroviral therapy 2 ) Cytomegalovirus retinitis 3 ) Ethambutol 4 ) HIV retinopathy 5 ) Toxoplasma retinitis
ANSWER: 3
5) A 26-year-old homosexual man presented to hospital with a fever, dry cough and dyspnoea. Oropharyngeal candidiasis was noted. He was found to be HIV antibody positive and Pneumocystis carinii was found on bronchoalveolar lavage. His Pneumocystis carinii pneumonia (PCP) was treated with intravenous co-trimoxazole and he was subsequently started on highly active antiretroviral therapy (HAART).Four weeks later he presented to clinic complaining of weakness and generalised aching. He was taking highly active antiretroviral therapy (zidovudine (AZT), lamivudine (3TC), nelfinavir), co-trimoxazole as Pneumocystis carinii prophylaxis and fluconazole.Investigations:Serum creatine kinase 700 IU/l (24-195)
What is the cause of this problem?
1 ) Co-trimoxazole 2 ) Fluconazole 3 ) Lamivudine (3TC) 4 ) Nelfinavir 5 ) Zidovudine (AZT)
ANSWER: 5

2 comments:
just an extra point, the organism Pneumocystis carinii has been renamed Pneumocystis jiroveci ,just in case some candidates get asked on this.
CDC has published an article named "A New Name (Pneumocystis jiroveci) for Pneumocystis from Humans" in 2002.
Full text can be found here
http://www.cdc.gov/ncidod/eid/vol8no9/02-0096.htm
To the author of this blog, keep up the good work.
Thank you for this extra information!
Post a Comment